
INTRODUCTION
Hypertension (HTN) is one of the most prevalent and modifiable risk factors for cardiovascular disease (CVD), contributing significantly to the burden of stroke, myocardial infarction (MI), chronic kidney disease (CKD), and premature mortality worldwide. In the United States (US), nearly half (measured as high blood pressure (BP) and/or taking antihypertensive medication) of adults aged ≥20 years have HTN.1,2 Between 2018 and 2023, HTN and its complications, such as hypertensive renal disease, accounted for a crude death rate of 12.7 per 100,000 population, highlighting its public health impact.3
According to the 2024 ACC/AHA statement on the management of HTN in the acute care setting, Systolic BP (SBP) ≥130 mm Hg or Diastolic BP (DBP) ≥80 mm Hg aligns with the definition of HTN.4 Asymptomatic elevated BP (AEBP), defined as SBP ≥130-180 mmHg or DBP ≥80-110 mmHg, is commonly seen in the inpatient setting. It is characterized by the absence of, symptom, sign, or diagnostic finding indicative of acute end organ damage, including but not limited to damage to the brain (eg, hypertensive encephalopathy, intracranial hemorrhage, and acute ischemic stroke), heart (eg, acute MI, unstable angina, acute left ventricular failure with pulmonary edema), large vessels (dissecting aortic aneurysm), kidneys, and the microvasculature.1,4 While hypertensive emergencies require urgent treatment, current evidence, including the 2024 ACC/AHA statement, recommends careful monitoring and addressing modifiable factors rather than immediate antihypertensive therapy in most cases, unless specific clinical reasons exist.4 The 2025 AHA/ACC HTN guidelines state that for adults with severe HTN (greater than 180/120 mmHg) who are hospitalized for noncardiac conditions and show no signs of acute target organ damage, it is not recommended to use additional intravenous (IV) or oral antihypertensive medications to reduce BP rapidly (level 3/harm).1 Factors related to acute illness or the hospital environment, such as pain, stress, sleep deprivation, withdrawal symptoms, missed home antihypertensive medications, and other drugs, can temporarily raise BP readings.5 Overtreatment of HTN may lead to adverse outcomes like hypotension, acute kidney injury (AKI), stroke, or myocardial injury.5,6 Treating Elevated BP in an inpatient setting is also associated with higher mortality rates and more extended hospital stays, which can, in turn, increase healthcare costs.6
Although target ambulatory BP ranges are well defined, evidence guiding inpatient BP thresholds remains limited.7 Consequently, variability in inpatient HTN management is common, often driven by inconsistent guidance to residents, hospitalists, and nursing staff, leading to unnecessary antihypertensive use and avoidable risk. This QI initiative evaluated AEBP management on the general medicine service at Trinity Health Oakland Hospital, implemented a structured multimodal educational program for multidisciplinary teams, and assessed post-education practice changes aimed at improving patient safety and guideline-based inpatient HTN care.
METHODS
Data source and study
This study was a retrospective, pre–post educational QI project utilizing a chart review design. The pre-education period (before education about the 2024 ACC/AHA recommendation) was from October to November 2024, and the post-education period was from May to June 2025.
Study Population
The adult patients aged ≥18 years admitted to the general medicine floors with AEBP, defined as a SBP 130-180 mmHg or DBP 80-110 mmHg, without symptoms or evidence of acute target organ damage.
Patients were excluded if they were admitted to intensive care units (ICU) or cardiac care units, admitted to non-medical floors such as surgery, obstetrics, or gynecology, had symptomatic HTN, or presented with hypertensive emergencies. Patients with asymptomatic markedly elevated BP (formerly hypertensive urgency) were excluded, as were those with cardiac conditions such as CVD, heart failure, valvular heart disease, or arrhythmias, including atrial fibrillation. Individuals with acute cerebrovascular accidents or transient ischemic attacks (TIAs), those undergoing active treatment for cardiac, cerebrovascular, or TIA, patients with CKD, pregnant patients, and those on comfort care were also excluded.
Sample Selection and Screening Process
Patients admitted to the general internal medicine floors who were discharged with an ICD-10 code for HTN (I10) and elevated BP without a history of HTN (R03.0). During the pre-education phase, 340 patient charts were screened, and 218 met the inclusion criteria, which were then fully reviewed. During the post-education phase, 264 patient charts were screened, with 176 meeting the criteria for full review (Figure 1).

Education about the ACC/AHA 2024 hypertension statement
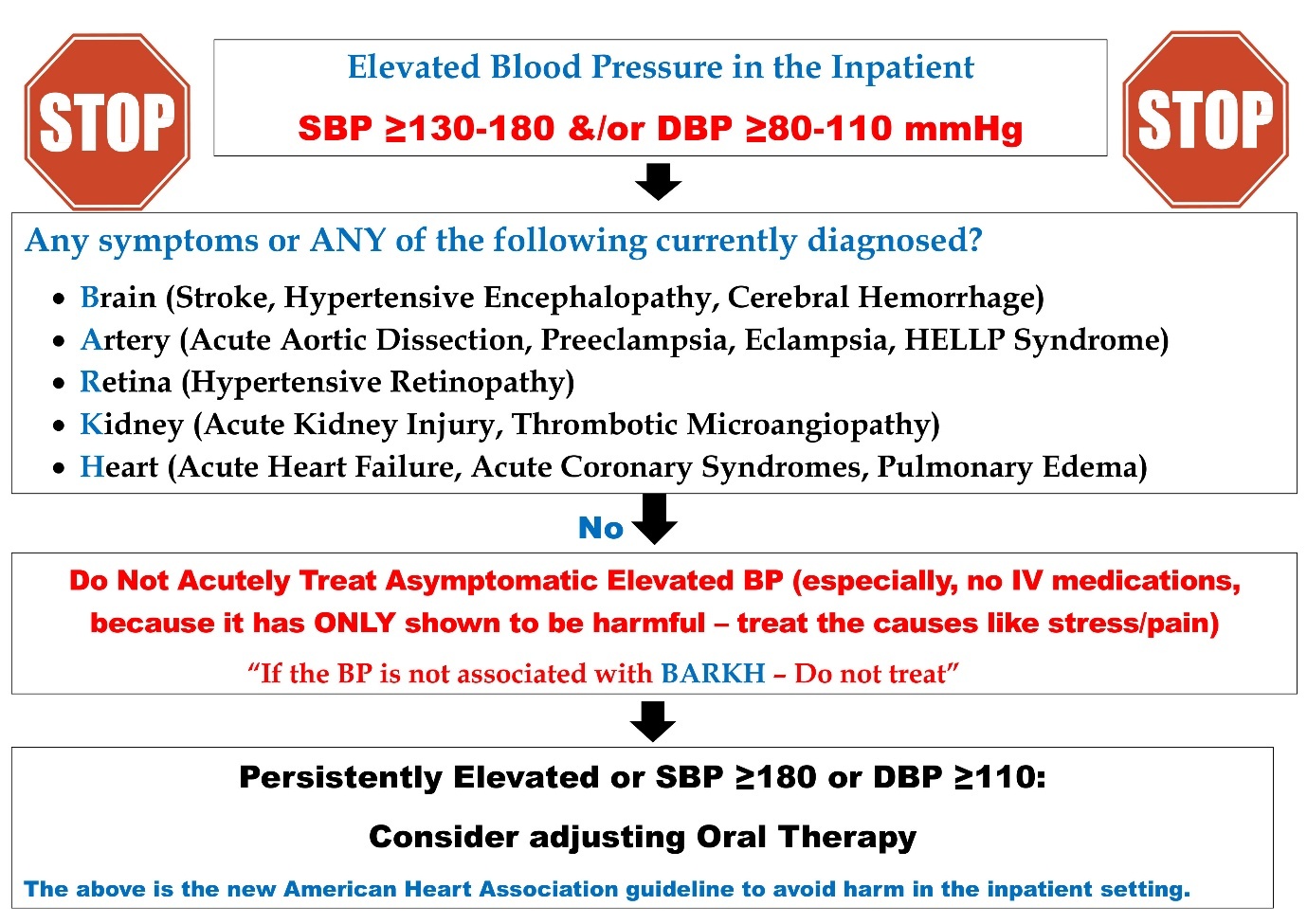
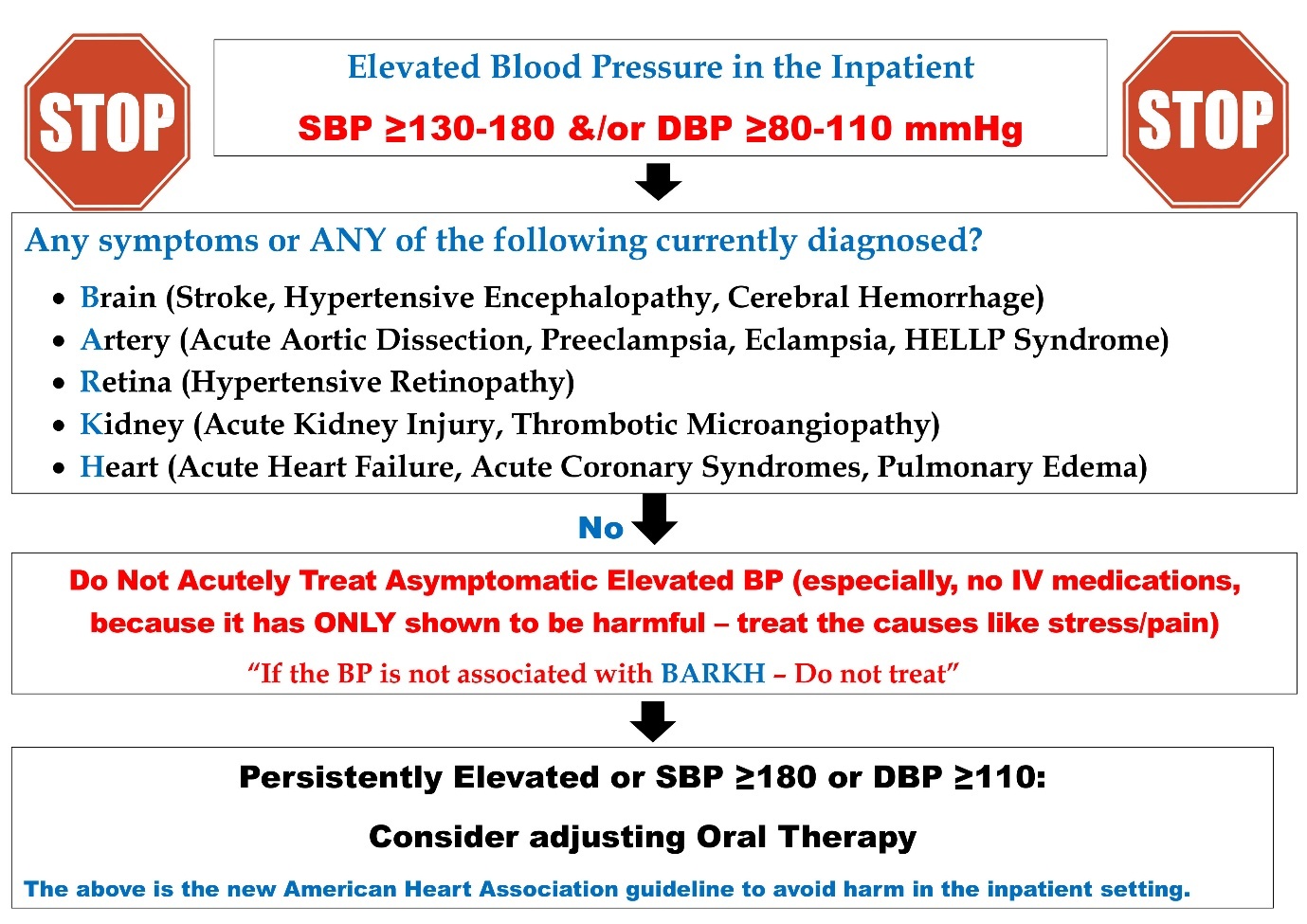
Between the two study periods, a structured, multi-modal educational intervention was implemented, targeting all members of the inpatient care team. The intervention consisted of noon conferences with internal medicine residents, nurse practitioners, physician assistants, and hospitalists, focusing on the 2024 ACC/AHA scientific statement on inpatient BP management. Nursing education campaigns were conducted, which included floor-to-floor teaching sessions and the distribution of printed pamphlets that guided appropriate BP thresholds for intervention, safe antihypertensive prescribing, and avoidance of unnecessary treatment in asymptomatic cases. Additional team-to-team presentations were delivered during handoffs and team meetings to reinforce best practices. Educational pamphlets were posted in common clinical work areas, including nursing stations, workrooms, and physician lounges, and the same educational materials were emailed to all care teams to ensure accessibility. The intervention emphasized evidence-based BP thresholds for treatment, safe medication administration, and prevention of complications such as hypotension and AKI (Figure 2).
Data Collection
Data was collected through review of patient charts by the internal medicine residents, and the information collected included patient demographics, admission diagnoses, pre-existing antihypertensive medication use, inpatient medication use, laboratory results, BP values before and after interventions, route of antihypertensive administration, and adverse outcomes.
Outcome Measures
The primary process outcome was the proportion of AEBP cases in which an antihypertensive medication was administered. Secondary outcomes included the change in BP after medication administration, the frequency of Pro Re Nata (PRN) antihypertensive administration, the route of administration, the incidence of AKI, post-intervention hypotension, and the proportion of patients experiencing a 25% or greater reduction in systolic BP after treatment. Hospital length of stay was also recorded.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation and compared using unpaired (Student’s) t-tests. Categorical variables were expressed as counts and percentages and compared using chi-square or Fisher’s exact test, as appropriate. A two-sided p-value of less than 0.05 was considered statistically significant. All analyses were conducted using SPSS version 28 (IBM Corp., Armonk, NY).
Institutional review board approval
Our study protocol was reviewed and approved by the institutional review board committee (THMR IRB #4) at our institution, Trinity Health Oakland Hospital, Pontiac, Michigan, United States (2024-055-THOA).
RESULTS
A total of 394 patients were included in the analysis, with 218 in the pre-education group and 176 in the post-education group (Figure 1).
Patient Demographics
The mean age was 59.7 ± 17.3 years in the pre-education group and 58.7 ± 17.8 years in the post-education group (p = 0.57). Males comprised 38.5% (n = 84) of the pre-education cohort and 39.2% (n = 69) of the post-education cohort (p = 0.89).
Race and ethnicity distributions were comparable between groups. White patients (69.7% vs 71.0%) and African American patients (23.9% vs 24.4%) comprised the majority of the cohort in the pre- and post-education periods, respectively, with no significant racial differences (p = 0.64). Most patients were not Hispanic/Latino (91.3% vs 85.8%), and overall ethnic distributions did not differ significantly between groups (p = 0.18) (Table 1).
Reason for Admission
Gastrointestinal disorders (25.6% vs 26.2%), infections (24.2% vs 25.0%), respiratory disorders (17.2% vs 17.4%), and other causes (29.3% vs 26.7%) accounted for the majority of admissions in the pre- and post-education periods, respectively, with no significant between-group differences (Table 1).
Hypertension History and Antihypertensive Use
A history of HTN was present in 53.7% (n = 116) of the pre-education group and 55.6% (n = 95) of the post-education group. Antihypertensive use at home was documented in 48.4% (n = 104) vs 45.2% (n = 76). The first BP reading consistent with HTN was observed in 68.3% (n = 218) versus 65.9% (n = 176). A change in discharge antihypertensive regimen occurred in 16.3% (n = 34) vs 12.8% (n = 20), and intensification of antihypertensive therapy at discharge occurred in 19.7% (n = 27) vs 12.7% (n = 20) (Table 1).
Baseline antihypertensive use, inpatient administration, and discharge prescribing patterns were similar between the pre- and post-education groups. No statistically significant differences were observed across major medication classes. Importantly, discharge antihypertensive intensification occurred less frequently in the post-education group (12.7% vs 19.7%), although this did not reach statistical significance (p = 0.136) (Table 1).
Laboratory Values
Baseline and discharge laboratory parameters, including serum creatinine, troponin, BNP, and potassium, were comparable between the pre- and post-education groups, with no statistically significant differences observed (Table 1).
Blood Pressure Metrics
BP parameters during hospitalization were similar between groups (Table 2). The only significant difference was a higher last DBP on the day of discharge in the post-education group (77.0 ± 13.1 mmHg vs 72.5 ± 12.9 mmHg; p < 0.001).
PRN Anti-hypertensive Intervention and Safety Outcomes
The proportion of patients receiving pharmacologic treatment for AEBP decreased significantly from 16.4% (35/214) in the pre-education period to 7.1% (12/168) post-education (p = 0.007). The frequency of PRN antihypertensive administration was similar between groups (54 vs 46 administrations; p = 0.91). Baseline BP at the time of treatment were comparable, with mean pre-education SBP of 159.5 ± 16.0 mmHg versus 156.1 ± 18.0 mmHg (p = 0.54) and DBP of 86.2 ± 14.7 mmHg versus 89.9 ± 19.5 mmHg (p = 0.50). Post-treatment BP responses were also similar, with no significant differences in first SBP or DBP following intervention (Table 3).
Among treated patients, the route of antihypertensive administration shifted significantly following the intervention (p = 0.041), with elimination of combined IV and oral therapy and an increase in oral-only treatment (28.6% pre vs 66.7% post), alongside reduced reliance on IV-only agents (40.0% vs 33.3%). Safety outcomes remained stable. A ≥25% reduction in SBP occurred in 8.6% of pre-education cases and 16.7% post-education. AKI temporally associated with antihypertensive administration was rare and did not differ between groups. Length of stay showed a nonsignificant downward trend from 4.96 ± 3.56 days to 4.61 ± 2.62 days (p = 0.28) (Table 3).
DISCUSSION
This single-center, pre–post QI study, using a structured, multidisciplinary education program aimed at residents, nurse practitioners, and nursing staff, reduced the use of pharmacologic treatment for asymptomatic inpatient BP elevation without evidence of harm. The proportion of patients with AEBP who received antihypertensives decreased from 16.4% pre-education to 7.1% post-education (p = 0.007). The last DBP on the day of discharge was significantly higher post-education (77.0 ± 13.1 mmHg) compared with pre-education (72.5 ± 12.9 mmHg, p < 0.001), reflecting less aggressive inpatient BP lowering. In addition, the route of antihypertensive therapy shifted significantly following the intervention (p = 0.041), characterized by increased oral-only treatment and elimination of combined IV and oral therapy. These findings align with contemporary guidance that distinguishes transient, context-driven inpatient BP elevations from true hypertensive emergencies and recommends careful reassessment and correction of modifiable contributors rather than reflexive drug therapy. The 2024 ACC/AHA Scientific Statement specifically cautions against routine treatment of asymptomatic inpatient BP and emphasizes process improvements over medication use in most cases, and our results demonstrate that focused education can effectively operationalize this guidance.4
Factors contributing to asymptomatic elevated BP
There are various reasons for elevated BP in the inpatient setting, including both patient- and hospital-environment-related factors.4 Pain, anxiety, drug intoxication, or drug or alcohol withdrawal, certain medications like NSAIDs, corticosteroids, decongestants, stimulants, erythropoietin, and calcineurin inhibitors can contribute to the elevated BP.1,4,8 In our study, more than 50% of the patients in both pre- and post-education phases had experienced either pain, agitation, or encephalopathy. We assessed the antihypertensives patients took at home and those they received during hospitalization (Table 1). Prior studies demonstrate frequent omission of home antihypertensive regimens during hospitalization, with 41% of patients prescribed PRN antihypertensives and 25% of postsurgical inpatients receiving IV antihypertensives not continued on their home medications.9,10 In addition, anti-hypertensive regimens might be altered on hospital admission because of formulary limitations, which can inadvertently affect their BP control during their hospitalization.4
Adverse outcomes of treating asymptomatic elevated BP with PRN medications
Among older adults hospitalized for noncardiac conditions, intensive inpatient blood pressure treatment has been associated with higher risks of a composite of mortality, AKI, stroke, myocardial injury, biomarker elevation, intensive care unit transfer, and hypotensive episodes.11 IV antihypertensive use increased the likelihood of a ≥30% reduction in mean arterial pressure by 40%,12 while PRN antihypertensive administration was associated with a twofold increase in mortality, a 24% higher risk of AKI, and a twofold risk of abrupt blood pressure lowering (>25% SBP reduction within 1 hour).5 Notably, 32.6% of patients receiving PRN IV antihypertensives experienced a >25% blood pressure reduction within 6 hours, often leading to downstream complications such as falls, syncope, tachycardia, and need for IV fluids.4,13–15 In addition, we have also observed a numerical reduction in the length of hospital stay, which wasn’t statistically significant: 4.96 ± 3.56 days during pre- versus 4.61 ± 2.62 days in the post-education phase, likely due to less overtreatment of AEBP and fewer medication-related complications. Our findings align with a growing body of evidence demonstrating that avoiding unnecessary inpatient BP treatment does not worsen outcomes and may reduce iatrogenic harm. Both IV and oral antihypertensive therapies have been associated with adverse outcomes across a range of BP levels, highlighting the need for caution when prescribing pharmacologic treatment for asymptomatic inpatient BP elevations.8,13,15–17
Management of asymptomatic elevated BP
Management of AEBP in the inpatient setting has been widely found to be associated with adverse in-hospital outcomes. Evaluation of inpatient BP should follow a systematic approach. First, assess for acute HTN-mediated organ damage, particularly when BP exceeds 180/120 mmHg, and manage hypertensive emergencies promptly in an intensive care setting. Next, confirm that proper measurement techniques were used, repeat readings after rest, and interpret nonstandard measurements cautiously.1,4,8,18 Elevated BP often reflects reversible contributors such as pain, anxiety, withdrawal, sleep deprivation, or physiologic stress, which should be addressed before initiating pharmacologic therapy.1,4,8,19–21 Medication reconciliation is essential to identify agents that may worsen BP and to reintroduce held home antihypertensives when appropriate. Finally, treatment decisions should be individualized, considering outpatient BP trends, comorbidities, age, frailty, and overall prognosis, as most patients with asymptomatic elevated BP do not benefit from inpatient regimen intensification.1,4,8,11,19,20,22 Furthermore, reviewing out-of-hospital BP readings, restarting the home regimen of antihypertensives, using oral formulations, especially in chronic HTN, and, in case of persistent elevation, recommending a medication change were recommended. In addition, a typical hospital stay is unlikely to be sufficient to assess the effect of a medication change.4
Discharge practices
Discharge practices are another vital consideration. At the time of discharge, a careful review and reconciliation of the medication, along with adequate patient counseling and planning for future care coordination, are important.4 It is also recommended to discharge the patient on a pre-hospitalization anti-hypertensive regimen4,6,11,14 and discontinue the medications that contribute to the elevated BP.4 It was also shown that adherence to the anti-hypertensive medication, which was initiated at the time of discharge, was low, and there was a low likelihood of getting refilled, or at least half of them were found to be discontinued by the end of a year.23 In our study, however, the intensification of antihypertensive therapy at discharge occurred in 19.7% of pre-education patients compared with 12.7% post-education. This is directionally consistent with findings from Anderson et al., who reported that discharge intensification among older adults did not improve long-term BP control but was associated with both adverse posthospital outcomes and low persistence to discharge medications.14,23,24 Arranging a follow-up in 2 weeks after discharge for comprehensive assessment, along with advising the patients to perform home BP monitoring, encouraging lifestyle modifications, medication adherence, and screening for the secondary causes of elevated BP, was recommended in case of clinical suspicion.1,4
Special Considerations
However, in certain groups, especially in those with persistently elevated BP, SBP/DBP >180/110–120 mm Hg, who have a history of high outpatient BPs, as well as those at a high risk for or with a history of CVD, treating elevated inpatient BP may be associated with more benefits than the risks.4 Priority should be given to fixed-dose or combination therapy, which helps promote medication adherence and effectively lower BP.1,4,25
Long-term Sustainability
The intervention succeeded by aligning evidence-based BP management with existing nursing and physician workflows. Education emphasized reassessing elevated readings, addressing reversible factors such as pain or anxiety, and distinguishing symptomatic from asymptomatic HTN. Integration of a BP algorithm into nursing communication and resident workstations supports sustained, consistent practice and reduces unnecessary escalation.
Strengths
This study was guideline-driven, multidisciplinary, and practical, achieving a significant reduction in unnecessary antihypertensive use without compromising safety. The educational intervention was low-cost, reproducible, and aligned with ACC/AHA recommendations, with favorable trends toward reduced discharge intensification and shorter hospital stay.
Limitations
Being a single-center pre–post study, the results are vulnerable to confounding and have limited generalizability. The sample size for treated patients was small, which reduced power for detecting rare outcomes. The reliance on ICD-10 coding, the lack of measurement audits, the absence of post-discharge outcomes, and the lack of subgroup or equity analyses further limit interpretation.
Clinical relevance
Findings indicate that structured education effectively reduces low-value inpatient HTN care, cuts down on overtreatment, and encourages safer, guideline-based practice without causing harm. Trends showing decreased IV use and discharge intensification further support its relevance to real-world clinical care.
Future Directives
Future studies should adopt multicenter, stronger designs, integrate EHR-based prompts and order sets, and evaluate broader outcomes, including readmissions, cardiovascular events, and costs. Subgroup and equity analyses, post-discharge monitoring, and ongoing audit-feedback cycles are essential to ensure lasting, equitable impact.
CONCLUSIONS
This QI initiative demonstrated that a structured, multidisciplinary educational intervention reduced unnecessary pharmacologic treatment of AEBP in hospitalized patients, reinforcing guideline-based recommendations for conservative inpatient BP management. Sustaining these gains through system-level integration and evaluating their impact on longer-term patient outcomes should be the focus of future efforts.
Author contributions
Conceptualization: Roopeessh Vempati (Supporting), Dinakaran Umashankar (Supporting), Muhammad Sanusi (Lead), Prami Nakarmi (Equal), Vivek Mittal (Supporting), Geetha Krishnamoorthy (Lead). Methodology: Roopeessh Vempati (Lead), Dinakaran Umashankar (Lead), Muhammad Sanusi (Lead), Quang Dat Ha (Equal), Utheja Dasari (Supporting), Vivek Mittal (Supporting), Geetha Krishnamoorthy (Lead). Project administration: Roopeessh Vempati (Supporting), Dinakaran Umashankar (Lead), Muhammad Sanusi (Supporting), Prami Nakarmi (Equal), Geetha Krishnamoorthy (Supporting). Resources: Roopeessh Vempati (Supporting), Dinakaran Umashankar (Supporting), Muhammad Sanusi (Supporting), Prami Nakarmi (Equal), Quang Dat Ha (Equal), Geetha Krishnamoorthy (Lead). Visualization: Roopeessh Vempati (Lead). Writing – original draft: Roopeessh Vempati (Lead), Dinakaran Umashankar (Lead), Muhammad Sanusi (Equal), Prami Nakarmi (Equal), Quang Dat Ha (Equal), Fathima Shehnaz Ayoobkhan (Equal), Utheja Dasari (Equal), Parjanya Bhatt (Equal), Geetha Krishnamoorthy (Equal). Supervision: Roopeessh Vempati (Equal), Dinakaran Umashankar (Equal), Muhammad Sanusi (Supporting), Utheja Dasari (Equal), Geetha Krishnamoorthy (Lead). Writing – review & editing: Roopeessh Vempati (Supporting), Dinakaran Umashankar (Equal), Muhammad Sanusi (Equal), Prami Nakarmi (Equal), Quang Dat Ha (Equal), Fathima Shehnaz Ayoobkhan (Equal), Utheja Dasari (Equal), Parjanya Bhatt (Equal), Vivek Mittal (Equal), Ihunanya Destiny Agomuoh (Equal), Geetha Krishnamoorthy (Equal). Data curation: Roopeessh Vempati (Equal), Dinakaran Umashankar (Equal), Muhammad Sanusi (Supporting), Prami Nakarmi (Lead), Quang Dat Ha (Supporting), Fathima Shehnaz Ayoobkhan (Supporting), Utheja Dasari (Supporting), Parjanya Bhatt (Supporting), Vivek Mittal (Supporting), Ihunanya Destiny Agomuoh (Supporting), Karen Hagglund (Supporting), Geetha Krishnamoorthy (Equal). Investigation: Roopeessh Vempati (Supporting), Dinakaran Umashankar (Lead), Muhammad Sanusi (Lead), Prami Nakarmi (Equal), Quang Dat Ha (Equal), Fathima Shehnaz Ayoobkhan (Equal), Parjanya Bhatt (Equal). Validation: Roopeessh Vempati (Equal), Muhammad Sanusi (Equal), Prami Nakarmi (Equal), Quang Dat Ha (Equal), Fathima Shehnaz Ayoobkhan (Supporting), Utheja Dasari (Equal), Karen Hagglund (Supporting), Geetha Krishnamoorthy (Equal). Software: Dinakaran Umashankar (Equal). Formal Analysis: Karen Hagglund (Lead).
Acknowledgements
We thank all the internal medicine residents (2024-2025), advanced practice providers, nurse practitioners, physician assistants, and nurses at our hospital, Trinity Health Oakland Hospital in Pontiac, Michigan, for the success of this quality improvement study.
Trinity Health Oakland Internal Medicine Residents: Kim Abbegail Tan Aldecoa, MD (kimabbegailtan.aldecoa@trinity-health.org), Tobiloba Ayodeji Bamigboje, MD (tobilobaayodeji.bamigboje@trinity-health.org), Samhitha Bitla, MD (samhitha.bitla@trinity-health.org), Jaisal Brar, MD (jaisal.brar@trinity-health.org), Sharanya Shre Ezhilarasan Santhi, MD (sharanyashre.ezhilarasansanthi@trinity-health.org), Kinjal Hirpara, MD (kinjal.hirpara@trinity-health.org), Muhammad Roohan Khan, MD (muhammadroohan.khan@trinity-health.org), Dhananja Meedeniya, MD (dhananja.meedeniya@trinity-health.org), Gaurav Mudgal, MD (gaurav.mudgal@trinity-health.org), Ayomide Ojo, MD (ayomide.ojo@trinity-health.org), Dakshin Padmanabhan, MD (dakshin.padmanabhan@trinity-health.org), Bhavin Patel, MD (bhavin.patel@trinity-health.org), Rahul Pidikiti, MD (rahul.pidikiti@trinity-health.org), Sumit Raut, MD (sumit.raut@trinity-health.org), Mahvish Renzu, MD (mahvish.renzu001@mercyhealth.org), Syeda Daniya Samreen, MD (syedadaniya.samreen@trinity-health.org), Yash Shah, MD (yash.shah@trinity-health.org), Fizza Zulfiqar, MD (fizza.zulfiqar@trinity-health.org), Syeda Juvaria Arshi, MD (syedajuvaria.arshi@trinity-health.org), Saba Asif, MD (saba.asif@trinity-health.org), Akashdeep Singh Grewal, MD (akashdeepsingh.grewal@trinity-health.org), Meumbur Praise Kpughur-Tule, MD (meumburpraise.kpughur-tule@trinity-health.org), Sangeetha Krishnamoorthy, MD (sangeetha.krishnamoorthy@trinity-health.org), Manohar Lal, MD (manohar.lal@trinity-health.org), Merfilius Leslie, MD (merfilius.leslie@trinity-health.org), Kshitij Mahajan, MD (kshitij.mahajan@trinity-health.org), Muhammad Muneeb, MD (muhammad.muneeb@trinity-health.org), Rishab Rajendra Prabhu, MD (rishabrajendra.prabhu@trinity-health.org), Hizqueel Ahmed Sami, MD (hizqueelahmed.sami@trinity-health.org), Ramneek Sandhu, MD (ramneek.sandhu@trinity-health.org), Shiv Shah, MD (shiv.shah@trinity-health.org), Nikhil Vojjala, MD (nikhil.vojjala@trinity-health.org), Ijaz Ali, MD (ali.ijaz@trinity-health.org), Kanika Goyal, MD (kanika.goyal@trinity-health.org), Chetna Hirani, MD (chetna.hirani@trinity-health.org), Aditya Kohli, MD (aditya.kohli@trinity-health.org), Nikhil Kumar Kotla, MD (nikhilkumar.kotla@trinity-health.org), Ngumimi Kpughur-Tule, MD (ngumimi.kpughur-tule@trinity-health.org), Ravi Kanubhai Patel, MD (ravi.kanubhaipatel@trinity-health.org), Rakshana Ravichandran, MD (rakshana.ravichandran@trinity-health.org), Reshma Reguram, MD (reshma.reguram@trinity-health.org), Assalah Brikho, MD (assalah.brikho@trinity-health.org), Rushi Shah, MD (rushi.shah@trinity-health.org), Tanisha Vora, MD (tanisha.vora@trinity-health.org), Kai Ying, MD (kai.ying@trinity-health.org)