Description of the clinical case
An 86-year-old woman (body mass index [BMI]26 kg/m²) with hyperthyroidism, poorly controlled type 2 diabetes mellitus, atrial fibrillation, sick sinus syndrome, non-ischemic dilated cardiomyopathy, and moderate–severe mitral regurgitation had a dual-chamber implantable cardioverter-defibrillator (ICD) placed in 2019 for cardiomyopathy. About 40 days before presentation, she sustained a periungual traumatic toenail injury during a pedicure.
She presented to the emergency department with 3 days of fatigue, tremor, and generalized weakness. On arrival, she was hypoglycemic (glucose 50 mg/dL) with subsequent fluctuations in glucose levels. Vitals showed low-grade fever and tachycardia; a new systolic murmur was noted on cardiac examination. The patient met systemic inflammatory response syndrome (SIRS) criteria with tachycardia (>90 beats/min) and leukocytosis; blood cultures were obtained.
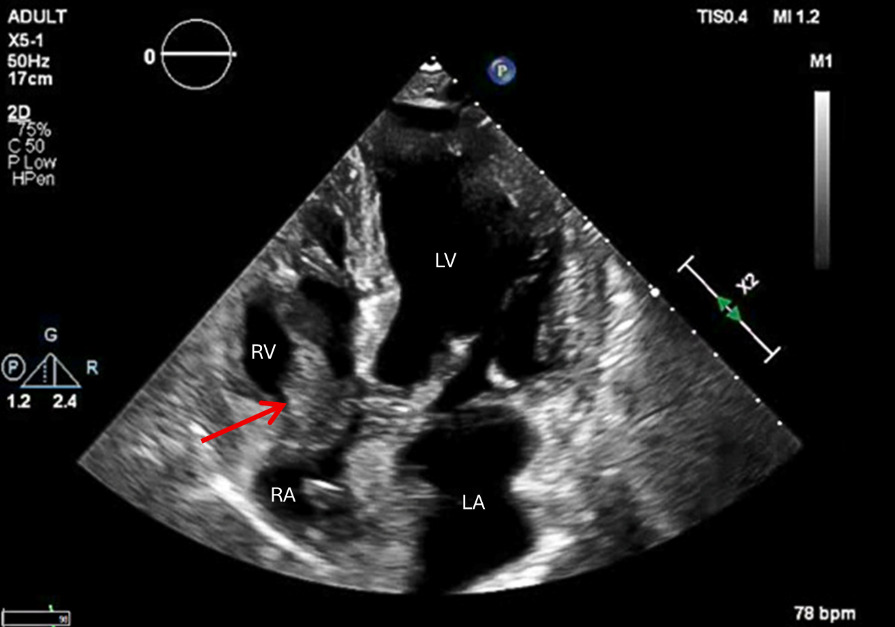
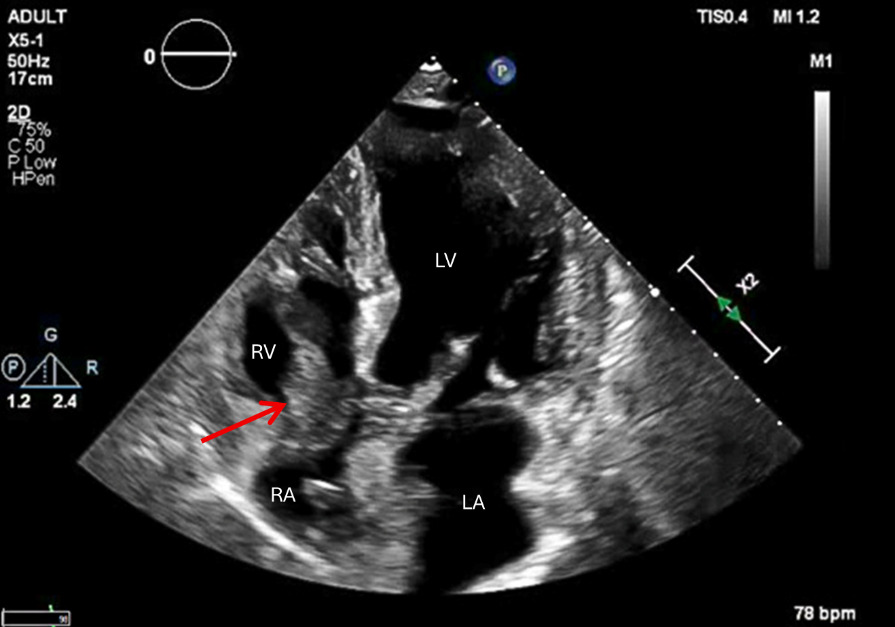
Three separate blood-culture sets subsequently grew Enterococcus faecalis. Transthoracic echocardiography (TTE, see Figure 1) revealed a large (40 × 20 mm), highly mobile echodensity attached to the right-atrial segment of the ICD lead and an 8 × 7 mm mass on the mitral valve. The right atrium was moderately dilated with persistent moderate–severe mitral regurgitation. Inspection of the device pocket showed no erythema or drainage. No definite source of Enterococcus faecalis bacteremia was identified. The recent periungual traumatic toenail injury was considered a possible, but unproven portal of entry.
What is your next course of action?
-
Vacuum-assisted debulking (AngioVac) followed by complete transvenous laser lead extraction.
-
Open-heart surgery (tricuspid vegetectomy with device extraction).
-
Start systemic anticoagulation to shrink the vegetation, with a delayed extraction.
Correct answer
# 1 – Vacuum-assisted debulking (AngioVac) followed by complete transvenous laser lead extraction.
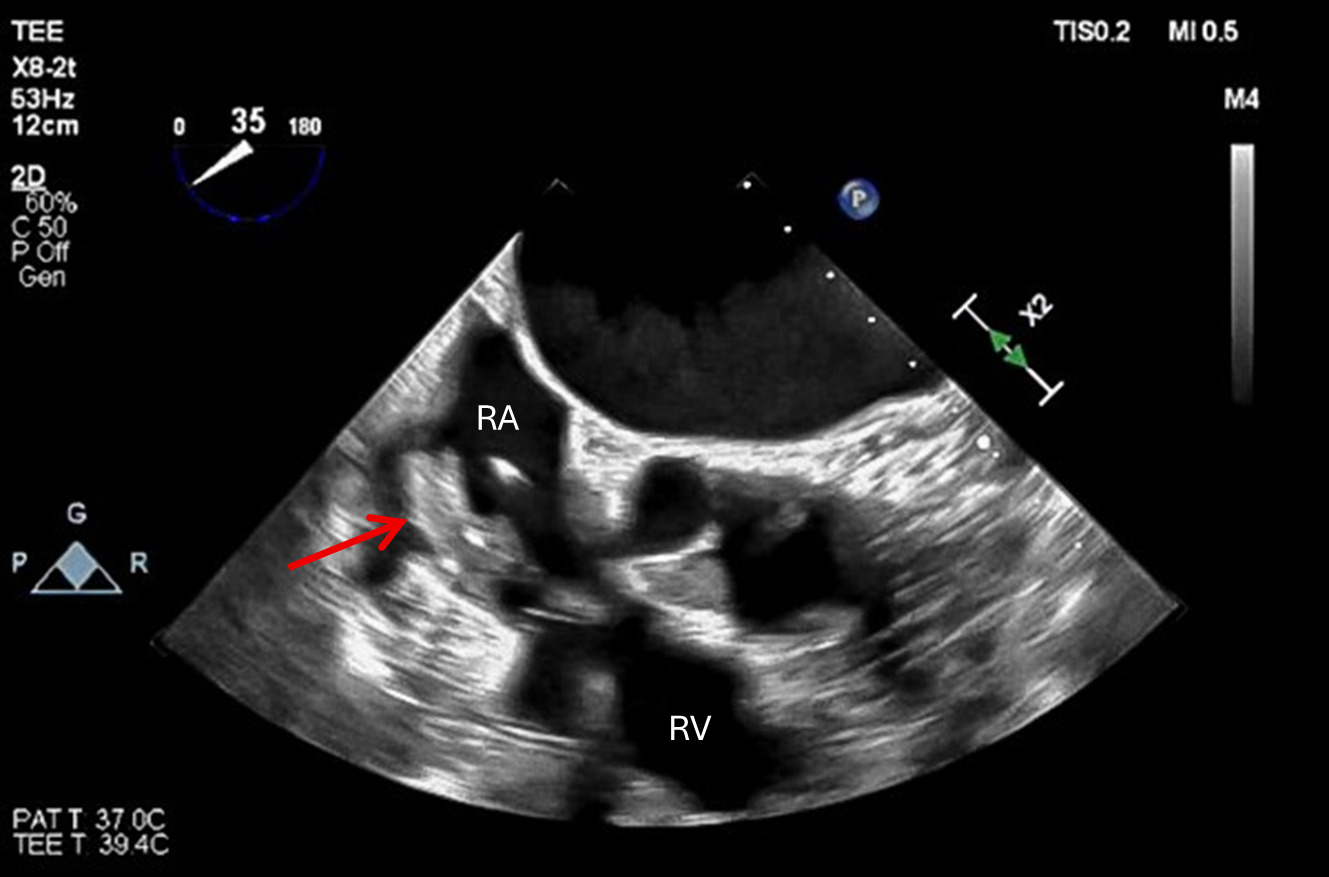
Transesophageal echocardiography (TEE)-guided vacuum debulking was the most appropriate first step given the giant (40 × 20 mm), highly mobile right-sided vegetation in this elderly patient with multiple comorbidities (Figure 2). AngioVac can reduce vegetation burden and lower embolic risk as a bridge to transvenous removal in elderly/high-risk patients when performed by experienced teams.1,2 This aligns with consensus that confirmed cardiovascular implantable electronic device (CIED) infection is not cured with antibiotics alone and ultimately requires hardware removal.1
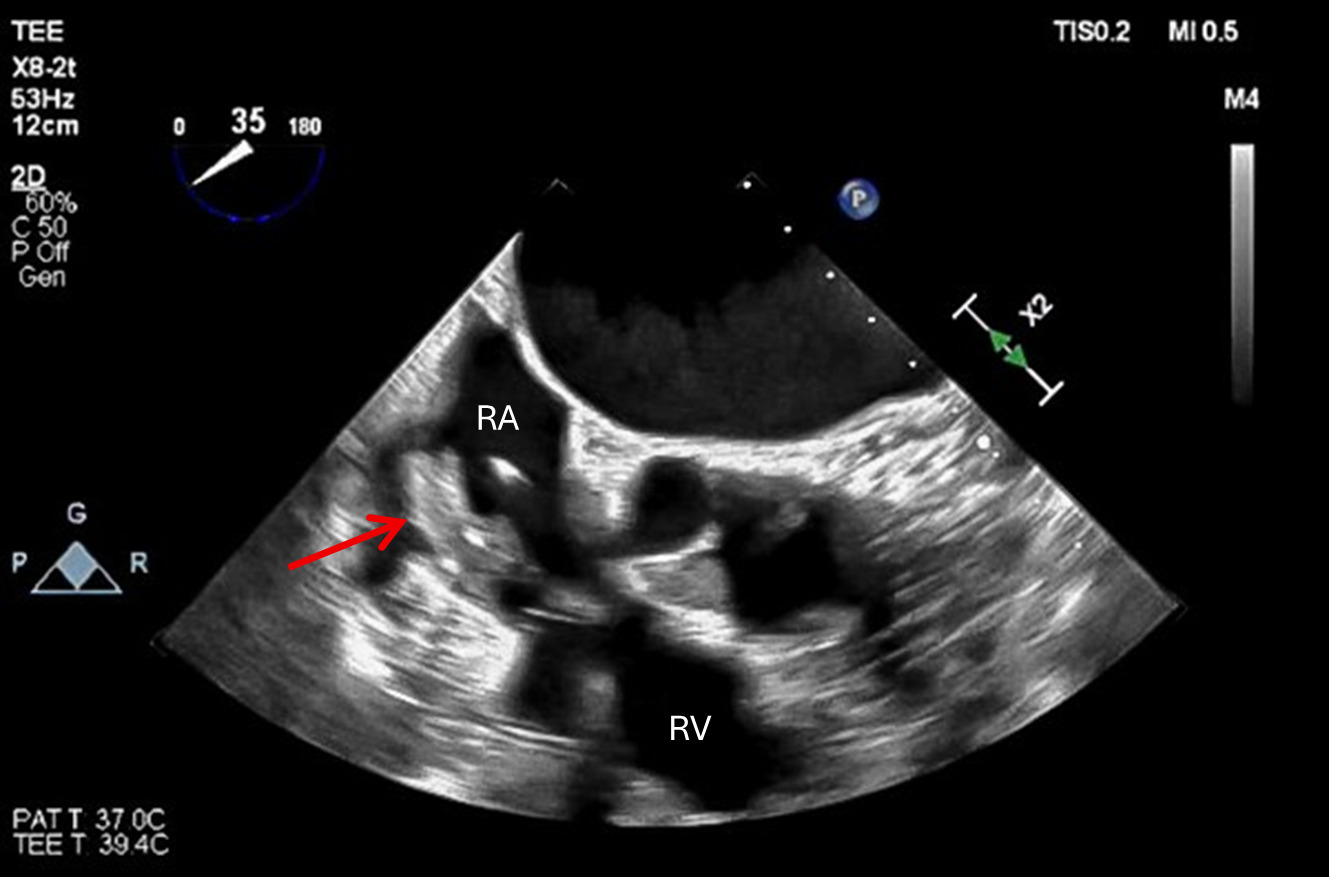
In our patient, intra-procedural TEE described a large, mobile pedunculated mass measuring 40 × 20 mm attached to the right-atrial lead that decreased to 26 × 15 mm after vacuum-assisted thrombectomy (debulking) but remained substantial and mobile. The team therefore progressed to laser-assisted transvenous lead extraction to achieve complete system removal, the definitive source-control step recommended once CIED infection is established.1 A staged, TEE-guided approach individualizes care, balancing embolic risk from a large, mobile vegetation with the patient’s frailty and comorbid moderate–severe mitral regurgitation (MR).1,3 In parallel, the mitral valve mass noted on TTE was treated as possible concomitant left-sided involvement, supporting a full course of Enterococcus faecalis–directed intravenous (IV) antibiotic therapy and planned follow-up echocardiography, while reserving mitral intervention for development of guideline-based surgical indications.3
Although there is no single universally “safe” vegetation size for transvenous extraction, embolic risk rises with increasing size and mobility, and consensus statements highlight larger lead masses (e.g., >20 mm, and particularly around >25 mm) as scenarios where open extraction may be considered and where additional risk-mitigation strategies are appropriate.1,4
This sequence—AngioVac debulk, then laser extraction under TEE guidance—provided the most evidence-aligned and risk-aware pathway to definitive source control in an octogenarian, consistent with frameworks that prioritize transvenous extraction and reserve surgery for specific indications (eg, heart failure from valve destruction, uncontrolled infection/abscess, recurrent embolization).1,3
Incorrect answers
# 2 Open-heart surgery first.
Initial sternotomy is not the default approach for isolated right-sided CIED infection without specific surgical indications (eg, refractory heart failure from valve destruction, uncontrolled infection/abscess, or recurrent emboli despite therapy).1,3 Transvenous extraction is generally first-line. In an octogenarian with multiple comorbidities and baseline MR, the operative risk is high while a percutaneous aspiration and extraction plan offers a safer, guideline-concordant alternative for very large vegetations when expertise is available.1,3
# 3 Start systemic anticoagulation to shrink the vegetation, with a delayed extraction.
Antibiotics do not eradicate biofilm on infected leads. Therefore, device retention carries high failure and relapse rates, and complete system removal is recommended once CIED infection is established.1,3On the other hand, anticoagulation does not treat infective vegetations or address infected hardware. It is not recommended as a strategy to “shrink” vegetations or justify deferring indicated extraction, particularly with a giant, mobile lead vegetation and documented bacteremia.1,3
Patient outcome
After ICD extraction, the patient was discharged with a peripherally inserted central catheter (PICC) to receive ampicillin-sulbactam 3 g IV four times daily plus gentamicin 80 mg IV once daily for 40 days. She was instructed to continue wearing a LifeVest (wearable cardioverter-defibrillator) as a temporary interim measure while re-implantation candidacy and timing were reassessed after infection clearance. Her insulin lispro (8 IU three times daily), insulin glargine (28 IU nightly), empagliflozin, lisinopril 5 mg, metoprolol 50 mg, and methimazole 5 mg daily were continued. Follow-up TEE at 3 months did not visualize residual vegetations. The previously described mitral lesion was no longer seen, which is consistent with interval healing. However, silent embolization or persistence of micro-vegetation cannot be fully excluded in the absence of interim imaging.
Discussion
This octogenarian with Enterococcus faecalis cardiac implantable electronic device–related infective endocarditis (CIED-IE) had a giant (40 × 20 mm) right-atrial ICD-lead vegetation but few early symptoms, underscoring the value of prompt echocardiography to define size, mobility, and anatomic risk. Successful treatment of CIED-IE requires definitive source control because biofilm limits the efficacy of antibiotics alone; contemporary guidance recommends complete system removal with pathogen-directed IV therapy when infection is established.1 Although the source of bacteremia was not definitively established, the recent periungual traumatic toenail injury was considered a possible, yet unproven portal of entry. However, this claim remained speculative and was not supported with solid evidence.
Given the very large, mobile right-sided vegetation and the patient’s advanced age/comorbidities, vacuum-assisted aspiration (AngioVac) was reasonable to debulk as a bridging method and reduce embolic burden before transvenous removal.2 After debulking, transvenous lead extraction (often laser-assisted) is the standard technique in experienced centers to achieve complete hardware removal, and extraction should not be deferred once CIED infection is confirmed.1 Open surgery is reserved for clear indications, such as heart failure from valve destruction, uncontrolled infection or abscess, or recurrent emboli.3. The 2023 European Society of Cardiology (ESC) guideline emphasizes multidisciplinary, patient-specific risk–benefit assessment. This is particularly important in older, frail patients, in whom less invasive approaches may reduce procedural risk while maintaining effective source control.3. Registry data further associate lead extraction with improved outcomes in device-related infective endocarditis (IE), supporting aggressive source control when feasible.5
Although the dominant pathology was the giant right-atrial ICD-lead vegetation requiring definitive source control via complete CIED removal, initial TTE also reported a small 8 × 7 mm mitral valve mass. The left-sided finding was treated as possible concomitant endocarditis and therefore directly informed the plan for full pathogen-directed IV therapy and scheduled follow-up echocardiography to document resolution or progression.3 At presentation, there were no ESC surgical indications for left-sided endocarditis (e.g., heart failure due to valve dysfunction, uncontrolled infection/abscess, or embolic-prevention surgery for large vegetations), and operative risk was prohibitive in this frail octogenarian.3 Percutaneous aspiration/debulking has the strongest published experience in right-sided and lead-associated lesions.2,3 For that reason, mitral debulking with embolic protection was not pursued. Surgical evaluation was reserved for persistent bacteremia, embolic phenomena, lesion enlargement, or worsening valve dysfunction.2,3
ICD re-implantation should typically follow infection clearance.1 Additionally, this should be coupled with reassessment of the ongoing ICD indication (primary vs secondary prevention), left ventricular ejection fraction (LVEF), any history of appropriate ICD therapies, and the patient’s frailty and overall clinical trajectory (which is particularly important in very elderly patients).1,3,6
In this context, the potential benefit of a wearable cardioverter-defibrillator (WCD) was temporary protection against sudden arrhythmic attacks during the mandated delay before any re-implantation decision, thereby avoiding premature reimplantation while infection clearance was being confirmed.3,6,7 However, this potential benefit must be balanced against several limitations of the use of WCD. Evidence supporting WCD use remains limited, especially in frail octogenarians. Its effectiveness also depends on adherence and tolerance. In older frail patients, the device may add practical burden, including discomfort, false alarms, skin irritation, and, rarely, inappropriate shocks.7 Therefore, WCD use should not be considered routine in this setting, rather, it may be considered selectively as a short-term bridge only when the treating team judges that residual arrhythmic risk is high enough to outweigh these burdens and limitations.3,7Finally, in our case, ICD re-implantation still required reassessment after extraction and infection clearance, and the WCD was used only as a short-term bridge, not as a predetermined plan for re-implantation.
Limitations
Staged debulking/extraction occurred at specialized centers, and very-late (>3-month) follow-up was unavailable.
Funding sources
No specific grant from funding agencies was received for this work.
Acknowledgment
We express our deep gratitude to the medical ward staff for their invaluable support in completing this report.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Data Availability Statement
De-identified data are available from the corresponding author upon reasonable request; source records are held by the originating private hospital.
Competing Interests
The authors have no competing interests to declare.
Permission to reproduce material from other sources
No materials were acquired from other sources.
Clinical trial registration
Not applicable in the scope of our research.
Author contributions
Conceptualization: Mustafa H Adleh (Lead), Ahmed M Saleh (Supporting). Investigation: Mustafa H Adleh (Equal). Writing – original draft: Mustafa H Adleh (Lead), Adel Mahmah (Equal). Writing – review & editing: Mustafa H Adleh (Equal), Raja H Rizwan (Supporting), Ahmed M Saleh (Supporting). Methodology: Mohammed AA Kassis (Lead). Data curation: Mohammed AA Kassis (Equal), Adel Mahmah (Supporting). Resources: Mohammed AA Kassis (Equal). Visualization: Mohammed AA Kassis (Lead). Validation: Raja H Rizwan (Lead). Supervision: Ahmed M Saleh (Lead). Project administration: Ahmed M Saleh (Lead).