INTRODUCTION
Coronavirus disease 2019 (Covid-19) infection is associated with an increased risk of venous thromboembolism (VTE).1 Though many early studies attempted to delineate a clear association between Covid -19 and VTE, due to the many comorbidities in the critically ill population studied as well as an increased rate of cytokine storm, it is unclear if Covid -19 itself is an independent risk factor for development of VTE in all Covid -19 cases, even those that do not require intensive care unit (ICU) care. Despite prophylactic use of anticoagulant therapy for Covid-19 patients, many still develop deep vein thrombosis (DVT) or pulmonary embolism. Klok et al. discovered that 27% of severe Covid-19 patients developed VTE despite thromboprophylaxis.2
Many studies investigating the relationship between Covid-19 and VTE have had varying results, prompting meta-analyses to aggregate the available data. These studies tended to look at the rates of thrombotic events in hospitalized patients, with a critical difference appearing to exist between those who were admitted to the hospital general floors and those who required admission to the ICU. Liu et al. found an incidence rate for VTE in overall hospitalized Covid-19 patients was 28.3% while patients admitted to the ICU had an incidence rate of 38.0%.3 Similar results were found in other meta-analyses suggesting that ICU admission was associated with a higher VTE incidence.4–9
Although ICU admission has been associated with higher VTE incidence in Covid-19 patients, it is unclear if mild Covid-19 infection is a significant risk factor for VTE. A case-control study investigating 661 patients with VTE from March 2020 through March 2021 found that mild Covid-19 infection was indeed a significant risk factor.10 Another recently published study, however, suggested that the overall incidence of VTEs in Covid-19 patients was lower than previously reported.11 Our goal was to investigate the overall incidence of VTE in patients with Covid-19 infection our community hospital and assess its associated risk factors.
MATERIALS AND METHODS
This study was approved by the Ascension Providence Hospital Institutional Review Board (IRBNet #1590494). We retrospectively reviewed the medical records of patients 18 years and older who presented to the emergency room at Ascension Providence Hospital and tested positive for Covid-19 using a nasopharyngeal swab for real-time polymerase chain reaction test between March 2020 and September 2021.
We collected demographic and clinical outcomes that included VTE and medical history. We performed descriptive analysis on the data, generating frequencies and percentages. We used IBM SPSS Version 26 (Armonk, NY) to analyze the data.
RESULTS
We found that 5926 patients aged 18 to 99 years tested positive for Covid-19 during this time period. Of these patients, 64 (1.08%) patients were discovered to have a VTE within two months of their Covid-19 diagnosis, with an average time between diagnoses of 9 days; 31 patients (48%) presented simultaneously with Covid-19 and VTE. Six (9%) were deemed mild cases of Covid-19 that did not require admission to the hospital and thus were discharged without prophylactic anticoagulation. Their VTE was discovered at a subsequent visit after an average of 19.8 days.
Males (n=40, 63%) were affected more frequently than females (n=24, 38%). The largest group affected was the African American population with a total of 37 individuals (58%, Table 1).
Of the 64 patients treated for VTE within 2 months of their Covid-19 diagnosis, 42 (66%) were patients requiring admission to the general hospital floor for hypoxia, acute respiratory failure, and acute kidney injury. Some of these patients (n=13, 31%) did not require medical prophylaxis, as their only risk factor was that they were in acute respiratory failure. Only 2 of the ICU-admitted patients were not initially treated prophylactically as well.
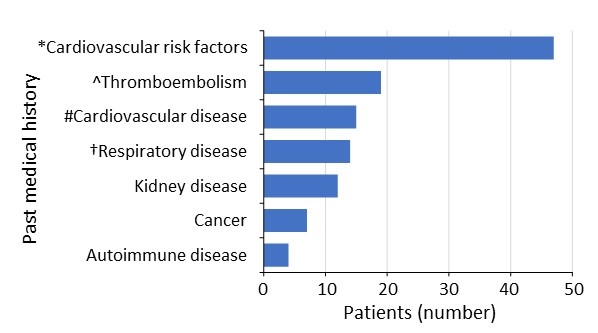
The highest number of VTE was seen in patients with a past medical history of cardiovascular risk factors (n=47, 73%) followed by a history of thromboembolism (n=19, 30%, Figure 1). Of the 64 patients, 20 (31%) expired, 30 (47%) were discharged home, and 11 (17%) were discharged to a medical facility.

DISCUSSION
Our study found that the total VTE incidence was 1.08%, as opposed to the general population’s rate of 0.1% (ten times higher).12 In our sample, more men were affected compared to women. African Americans represented the highest percentage of VTE occurrence, which was consistent with our hospital’s patient demographics. Covid-19 infection, even mild category, not requiring hospitalization, was a risk factor for VTE. We found that the top two risk factors for VTE associated with Covid-19 infection were presence of cardiovascular risk factors and prior history of thromboembolism.
It is essential to underscore that lack of awareness to risk factors of VTE in general contribute significantly to increased incidence. Specifically, those patients who were admitted with acute respiratory failure (have increased need for oxygen and immobility), were classified as being in a moderate-risk category for VTE. Despite meeting at least two criteria, only 50% of patients who satisfied these criteria were provided with medical prophylaxis for VTE.13
Our study’s limitations included its sample size, the variation in VTE prophylaxis, and frequent changes in the standards of care throughout the Covid-19 pandemic. For example, due to lack of evidence, patients with mild Covid-19 infection did not receive anticoagulation. On the other hand, patients with moderate to severe Covid-19 infection were treated prophylactically with anticoagulation.
Therefore, there was variation in VTE prophylaxis among patients with Covid-19 infection even after the development of clinical guidelines.14 Additional risks to VTE are associated comorbidities from the severity of Covid-19 infection. For example, patients in acute hypoxic respiratory failure are also immobilized, which could be a major contributory factor to the increased risk of development of VTE. However, what is reported in this study and requires further investigation is why mild cases of Covid-19 were presenting with unexpected VTE days later after testing positive despite no known associated risk factors (hospitalization or immobilization). These questions are important to explore so that we can modify practice guidelines for VTE prophylaxis, if necessary, given the implications of VTEs on the patient’s overall health.
CONCLUSIONS
In our population of Covid-19 patients, the VTE incidence was higher than the general population. Though our study has a limited sample size, it supports the belief that mild Covid-19 infection not requiring hospitalization is a risk factor for VTE, and further studies regarding prophylactic anticoagulation in this population are warranted.
ACKNOWLEDGEMENTS
The authors would like to thank all the volunteers, students and residents from Ascension Providence Hospital who have helped in the data collection in the Covid-19 registry. Also special thanks to Dr. Joseph Gardiner, a distinguished professor from Michigan State University College of Human Medicine, for his overall assistance in the data registry of this cohort.
CONFLICT OF INTEREST DISCLOSURE
The authors report no sources of funding or conflicts of interest.
AUTHOR CONTRIBUTIONS
Conceptualization: Radwa Koujane (Supporting), Julia Pudar (Supporting). Investigation: Radwa Koujane (Lead), Julia Pudar (Supporting), Ryan Fernandez (Supporting). Writing – original draft: Radwa Koujane (Lead). Methodology: Nancy M Jackson (Supporting), Abdulghani Sankari (Lead). Formal Analysis: Nancy M Jackson (Lead). Data curation: Jeffrey C Flynn (Lead). Writing – review & editing: Jeffrey C Flynn (Supporting), Abdulghani Sankari (Supporting). Supervision: Abdulghani Sankari (Lead). Project administration: Abdulghani Sankari (Lead).
CORRESPONDING AUTHOR:
Abdulghani Sankari, M.D., Ph.D.
Professor & Director of Medical Education Department/DIO
Ascension Providence Hospital
Wayne State University School of Medicine
Michigan State University College of Human Medicine
16001 West Nine Mile Rd
Southfield, MI 48075
Work phone: 248-849-5525
Work fax: 248-849-5323
Email: abdulghani.sankari@ascension.org